Search our site for

How endometriosis affects fertility and pregnancy
Key facts
What is endometriosis?
Endometriosis is a chronic (long-term) inflammatory condition where tissue similar to the lining of the uterus (the endometrium) grows outside the uterus.
This tissue can grow on the:
- ovaries
- fallopian tubes (the tubes that allow eggs to travel from the ovaries to the uterus)
- lining of the pelvis
- bowel or bladder
- ligaments supporting the uterus
Similar to normal endometrial tissue, it responds to hormones during the menstrual cycle. But because it grows outside the uterus, it has no way to leave the body during a period. This can cause:
- inflammation
- scarring (adhesions)
- cysts on the ovaries (endometriomas)
Some women have few or no symptoms — they may not even know they have endometriosis. Others experience severe symptoms that affect their quality of life. Common symptoms include:
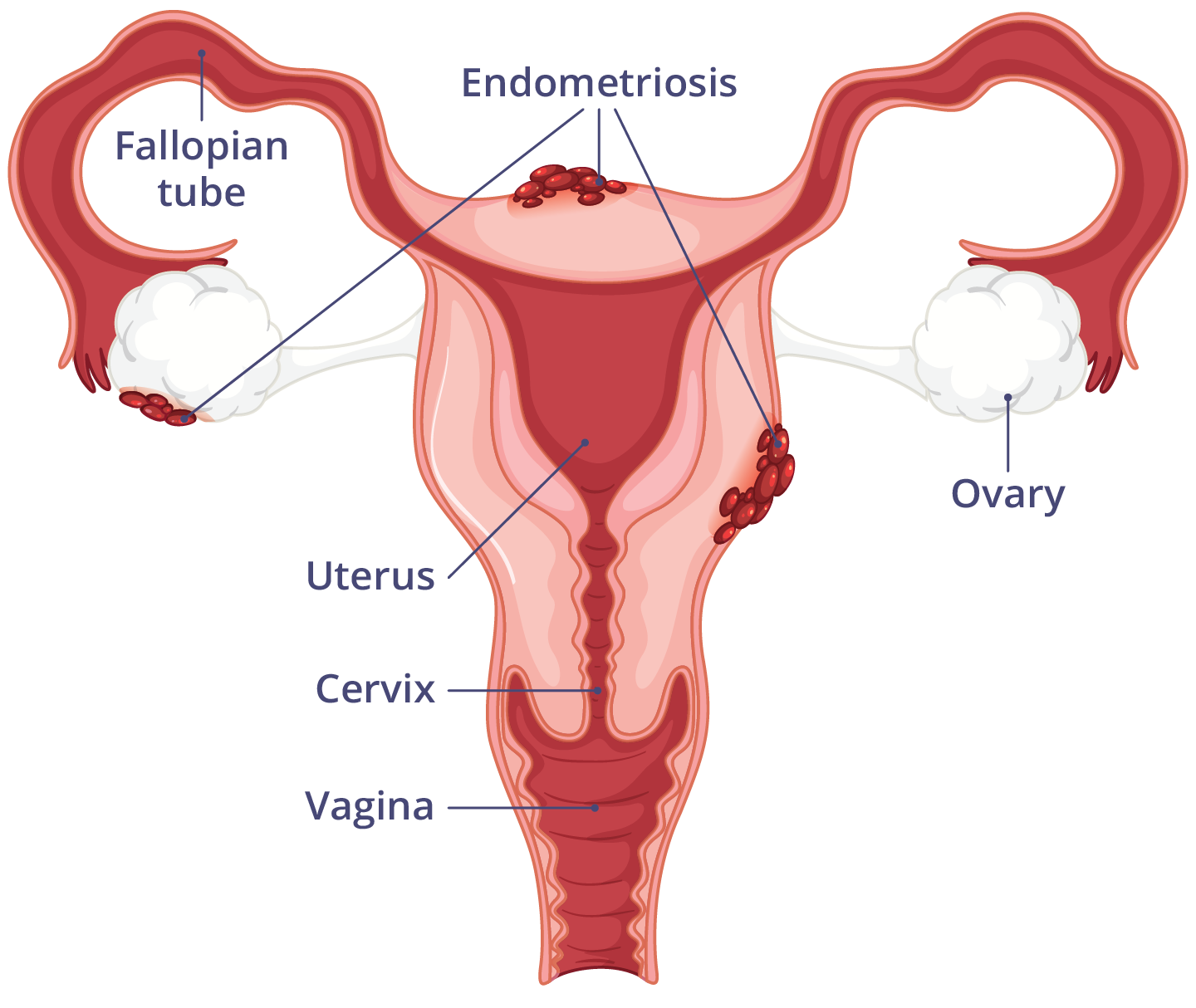
Endometriosis occurs when a layer of tissue, similar to that lining the uterus, grows outside it.
Can endometriosis affect fertility?
Yes — endometriosis can affect fertility. While many women with endometriosis fall pregnant naturally, around 1 in 3 women with endometriosis have trouble getting pregnant.
Endometriosis can affect both natural conception and assisted fertility treatments, such as in vitro fertilisation (IVF). It may impact fertility by:
- affecting how an egg develops in the ovaries or how it is released
- reducing egg quality
- causing hormone imbalances after ovulation (luteal phase problems)
- lowering fertilisation rates
- affecting early embryo development
Although it can be harder to become pregnant, most women with endometriosis are still able to have children.
Can endometriosis affect my pregnancy?
While most women with endometriosis have healthy pregnancies, there is a slight increase in the risk of some complications. These include:
- pregnancy loss (miscarriage) or ectopic pregnancy
- having a baby who is small for their gestational age
- caesarean birth (C-section)
- heavy bleeding (haemorrhage)
- preterm birth (before 37 weeks)
- placenta problems such as placenta previa
- hypertensive disease of pregnancy, including pre-eclampsia
Even if the risk is a little higher, most women with endometriosis have healthy pregnancies. Early and regular antenatal care helps monitor for any concerns.
Read more about staying healthy while you are pregnant.
How can endometriosis be treated during pregnancy?
Your doctor may recommend hormonal medicines such as the oral contraceptive pill ('the pill'), a contraceptive implant or an intrauterine device to treat endometriosis. These treatments can't be used during pregnancy, and you will need to stop them before trying to have a baby, either naturally or through IVF.
Some people experience improvement in symptoms during pregnancy due to hormonal changes. Others may continue to have pain.
Pain management options during pregnancy are limited and should always be discussed with your doctor, midwife or pharmacist. Always check before taking any medicines if they are safe to use in pregnancy.
Other treatment options may include:
- physiotherapy
- psychological interventions such as mindfulness, psychotherapy or counselling
- dietary changes
- acupuncture
Does endometriosis affect giving birth?
Endometriosis can make a caesarean birth more likely, but it does not mean you will need one. Most women can still plan for a vaginal birth, unless there is a medical reason for a caesarean.
Your healthcare team will consider your medical history, monitor your pregnancy closely and talk with you about the best birth options for you and your baby. Through a process of shared decision-making, they will help you make informed decisions and plan the safest and most suitable birth.
Will I still have endometriosis after having a baby?
Yes — there is no cure for endometriosis. Many women experience improved symptoms during pregnancy, but symptoms often return once periods restart, breastfeeding reduces or stops, or hormone levels return to their usual cycle. Symptoms can return at different times for different people.
Caring for yourself after birth when you have endometriosis
The postpartum period involves major physical and hormonal changes. If you have endometriosis, understanding what to expect can help you plan for this time.
What to expect after birth
After birth, hormone levels of the hormones oestrogen and progesterone drop quickly. Your period may return within weeks if you are not breastfeeding, or several months later if you are. Every person is different.
Breastfeeding, hormones and symptom changes
Breastfeeding changes your hormone levels. For some women, this can reduce endometriosis symptoms, including pain and risk of symptom recurrence. The improvement may last longer if you breastfeed for longer, but this is different for everyone. Symptoms often return once periods resume.
Breastfeeding should always be based on what feels right for you and your baby.
Managing endometriosis after birth
After pregnancy, you may wish to review your long-term management plan for endometriosis. Options may include:
- hormonal contraception
- progestogen therapies
- pain management strategies
- physiotherapy
- seeing a specialist to talk about surgery if your symptoms are severe
If you are considering future pregnancies, discuss timing and treatment options with your doctor or gynaecologist.
Mental and emotional wellbeing
Living with endometriosis can be emotionally challenging, particularly if you have had trouble getting pregnant or have had pregnancy problems.
After birth, it's common to feel emotional. You may experience:
- anxiety
- low mood
- stress
- baby blues
Caring for a newborn while being in pain can feel overwhelming. You don't need to manage this alone. You can get support from:
- your partner, family or friends
- your GP
- your child health nurse
- a psychologist or counsellor
- support groups for parents
- endometriosis support organisations
Looking after your mental health is an important part of your recovery.
Resources and support
Endometriosis and pelvic pain clinics are now being established and are funded by the Australian Government Department of Health, Disability and Ageing.
You can also visit Endometriosis Australia to:
- find resources about endometriosis
- keep up to date on endometriosis research
- find support groups and learn about clinics near you
Languages other than English
Jean Hailes for Women's Health offers fact sheets in a variety of languages.
The Royal Women's Hospital has a range of fact sheets on women's health topics in different languages.
Information for sexually and gender-diverse families
Endometriosis Coalition provides information about endometriosis for gender-diverse people.
Endometriosis Australia has an article and video on gender-affirming endometriosis care.
Information for Aboriginal and/or Torres Strait Islander peoples
Institute for Urban Indigenous Health offers a culturally safe Pelvic Pain and Endometriosis Management Program for Aboriginal and/or Torres Strait Islander peoples, including a 'Find a clinic' tool.
Visit the Strong Women, Strong Babies, Strong Culture Program, developed by the National Aboriginal Community Controlled Health Organisation (NACCHO).

Speak to a maternal child health nurse
Call Pregnancy, Birth and Baby to speak to a maternal child health nurse on 1800 882 436 or video call. Available 7am to midnight (AET), 7 days a week.
Find out how we develop and review our content.
Last reviewed: February 2026